For patients living in Japan
Surgical procedures
Various types of treatment options
are available.
are available.
Our priority is to provide the most suitable treatment options for each individual patient according to their personal wishes and needs.
Low back Surgery
Treatment types about our group's low back surgeries
Our group performs almost all low back surgeries endoscopically. Endoscopic surgery is a procedure characterized by small wounds, minimal muscle damage, and low risk of wound infection. In addition to endoscopic surgery, there are other treatment options such as laser therapy (PLDD) and Hernicore®.
| Operative procedure | Method of anesthesia | Length of hospital stay | Wound size | Indications |
|---|---|---|---|---|
| MED/MEL | General anesthesia | 4-6 days | 18-20 mm x one site | LDH*1, LSCS*2 |
| FED/FEL | General anesthesia | 3-4 days | 8-10 mm x one site | LDH, LSCS |
| Fusion surgery | General anesthesia | 8-10 days | 18-30 mm x one site 12 mm x four sites | Spondylolisthesis, LSCS, LDH (accompanied by instability) |
| PLDD | Local anesthesia | Day procedure | Needle hole | LDH |
| Hernicore® | Local anesthesia | Day procedure | Needle hole | LDH |
*1 LDH : Lumbar Disc Herniation
*2 LSCS : Lumbar Spinal Canal Stenosis
*2 LSCS : Lumbar Spinal Canal Stenosis
MED/MEL Microendoscopic Discectomy / Microendoscopic Laminectomy
Most common surgical procedure for low back
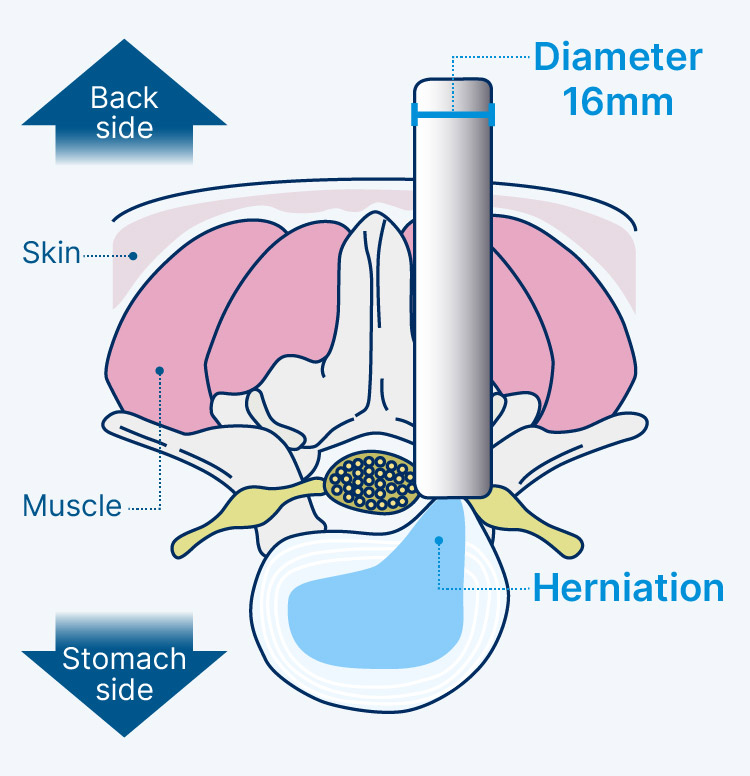
Both MED and MEL are surgical procedures performed while viewing the surgical field with an endoscope. MED is a procedure to remove a herniated lumbar disc. MEL is a technique used for lumbar spinal canal stenosis. The vertebral arch and yellow ligament are removed and the narrowed spinal canal is widened to relieve nerve compression. An endoscope is inserted from the back of the body. The outer tube into which the endoscope is inserted is 16 mm in diameter, which results in a wound about 20 mm in size.| Indications | Lumbar disc herniation (MED), lumbar spinal canal stenosis (MEL), etc. |
|---|---|
| Method of anesthesia | General anesthesia |
| Length of hospital stay | 4-6 days |
| Wound size | 18-20 mm x one site |
FED/FEL Full-endoscopic Discectomy / Full-endoscopic Laminectomy
Surgical procedure using a 7mm endoscope
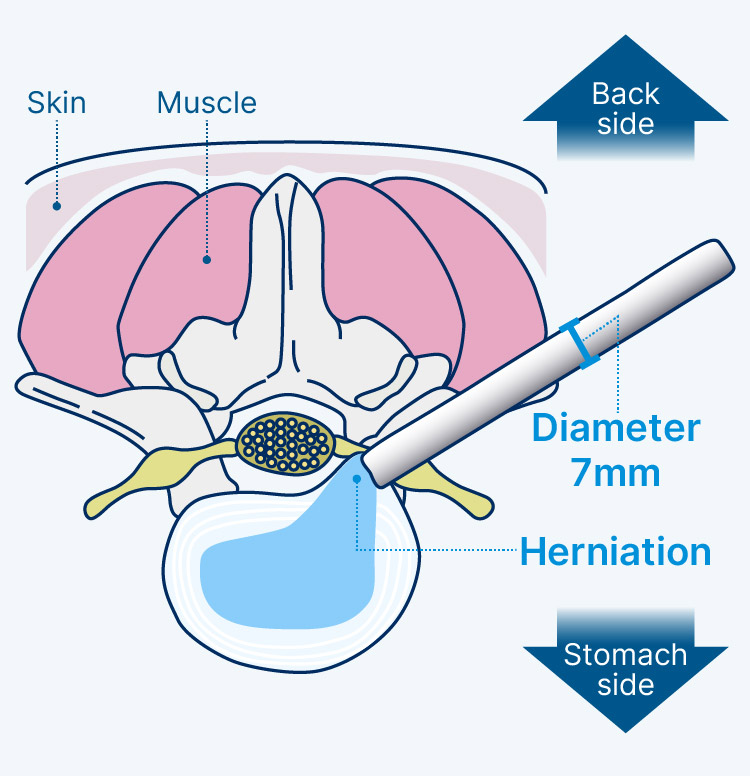
Both FED and FEL are surgical procedures performed while viewing the surgical field with an endoscope. FED is an operation to remove a herniated lumbar disc. FEL is a technique used for lumbar spinal canal stenosis. The vertebral arch and yellow ligament are removed and the narrowed spinal canal is widened to relieve nerve compression. The outer tube into which the endoscope is inserted is 7 mm in diameter, which results in a wound less than 10 mm in size.FED and FEL are a type of surgical procedure called FESS (Full-endoscopic Spine Surgery). FESS uses a spinal endoscope, which is not easy for the surgeon to manipulate. Although there are only a limited number of doctors in Japan who can perform FESS, many of the doctors in our group are proficient in the procedure.
| Indications | Lumbar disc herniation (FED), lumbar spinal canal stenosis (FEL), etc. |
|---|---|
| Method of anesthesia | General anesthesia |
| Length of hospital stay | 3-4 days |
| Wound size | 8-10 mm x one site |
UBE/BESS Unilateral Biportal Endoscopy / Biportal Endoscopic Spine Surgery
Latest surgical procedure by biportal
In conventional surgery, an endoscope is inserted through a single wound. In this technique, which has become popular in recent years, the operating instrument is inserted through another small hole in addition to the endoscope. The size of each wound is about 5 to 10 mm, smaller than those caused by the MED/MEL procedures. As with FED/FEL, this operation is performed with water irrigation. This technique is easier for surgeons to perform and is expected to become more popular in the future.| Indications | Lumbar disc herniation, lumbar spinal canal stenosis, etc. |
|---|---|
| Method of anesthesia | General anesthesia |
| Length of hospital stay | 3-4 days |
| Wound size | 5-10 mm x 2 sites |
Lumbar interbody fusion
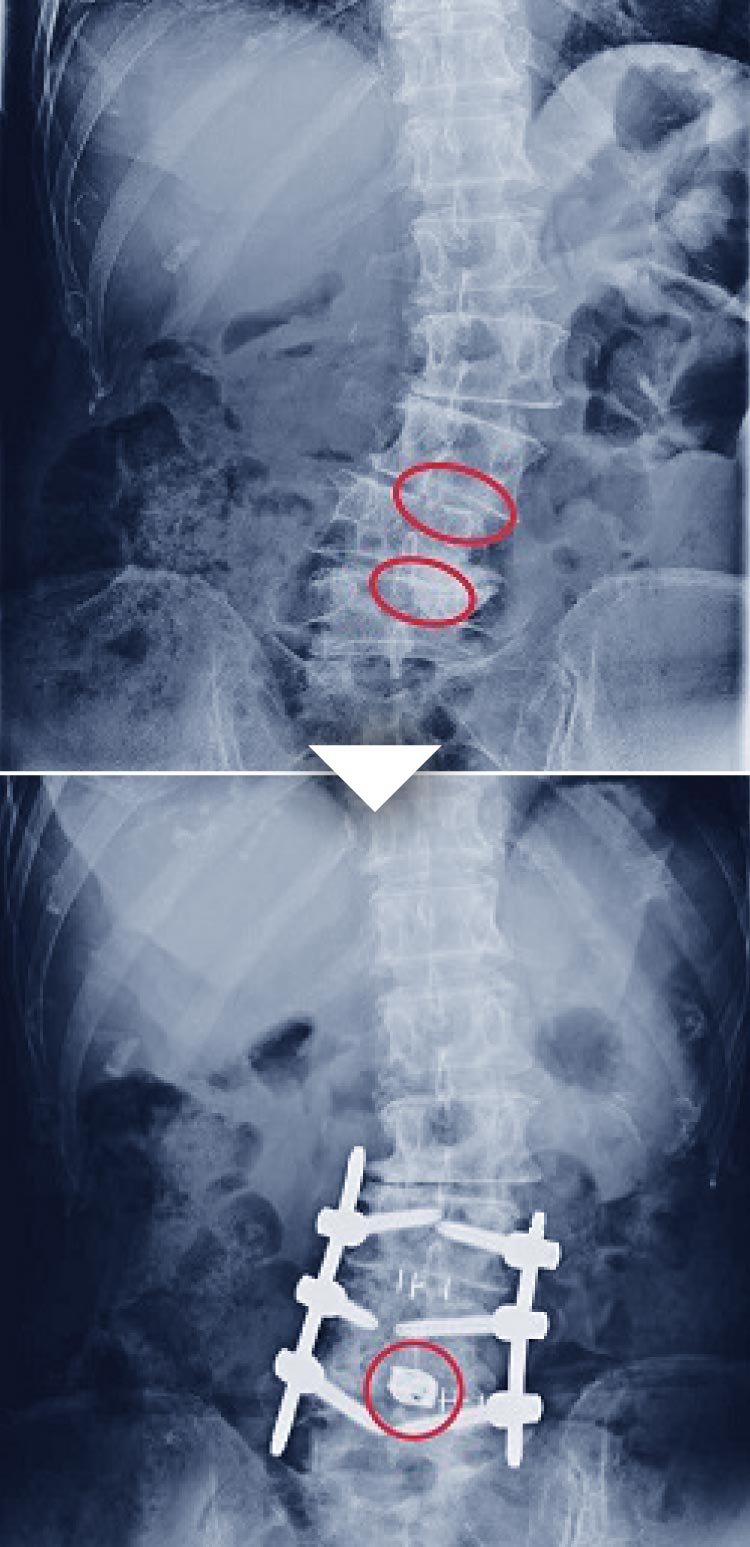
Surgical procedure to stabilize the spine by fixing part of the spine
Lumbar interbody fusion is a procedure in which two or more bones are connected by screws or other means. Fusion surgery is often chosen for spondylolisthesis, which is a misalignment of the spine; vertebral canal stenosis, which is a narrowing of the nerve pathway next to the spine; and severe discogenic pain. Screws are used to fix the spine so that the narrowed nerve pathway will not move; if it is discogenic, the disc is removed and fixed to prevent symptoms from occurring. The disadvantage is that Lumbar interbody fusion is more invasive than surgery without fusion. However, our group treats only the affected area based on accurate and precise diagnosis.Therefore, even if Lumbar interbody fusion is required, we will minimize the amount of intervertebral fusion as much as possible.
| Indications | Degenerative lumbar spondylolisthesis/ spondylolytic spondylolisthesis, lumbar spinal canal stenosis, lumbar disc herniation, etc. |
|---|---|
| Method of anesthesia | General anesthesia |
| Length of hospital stay | 8-10 days |
| Wound size | 18-30 mm x one site + 12 mm x four sites |
PLDDPercutaneous Laser Disc Decompression
Surgical procedure to decompress the intervertebral disc with a laser
PLDD is a treatment for lumbar disc herniation, in which a laser fiber is inserted into the disc space and the laser energy emitted by the fiber is used to vaporize and ablate the nucleus pulposus.| Indications | Lumbar disc herniation |
|---|---|
| Method of anesthesia | Local anesthesia |
| Length of hospital stay | Day procedure |
| Wound size | About the size of a needle hole |
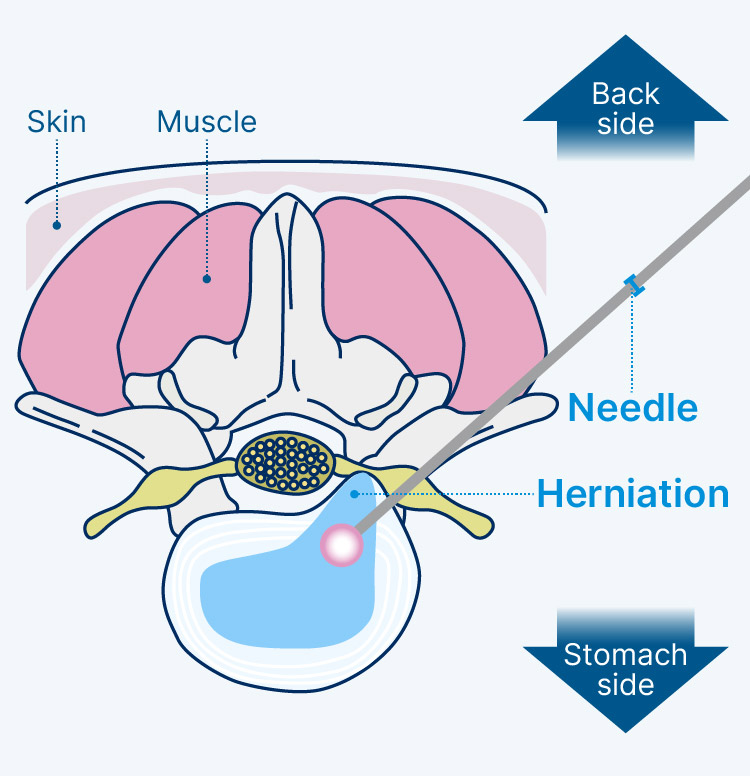
Hernicore®
This is a new treatment for lumbar disc herniation. An enzyme made from bacteria is injected into the nucleus pulposus, causing the protruding nucleus pulposus to retract into the disc. Currently, treatment with Hernicore® is available only in Japan.
Neck Surgery
Treatment types about our group's neck surgeries
Our group performs about half of all neck surgeries endoscopically. Non-endoscopic procedures are also minimally invasive. All neck surgeries are performed under general anesthesia.
| Operative procedure |
Endoscope | Length of hospital stay |
Wound size | Indications |
|---|---|---|---|---|
| MECD/MECL | Used | 4-6 days | 18-20 mm x one site | CDH*1, CSCS*2, cervical spondylosis, etc. |
| FECF | Used | 3-4 days | 8-10 mm x one site | CDH, cervical spondylotic radiculopathy, etc. |
| Cervical laminoplasty | Not used | 5-9 days | 50-80 mm x one site | CSCS, cervical myelopathy, etc. |
| Anterior cervical fusion | Not used | 7-10 days | 30 mm x one site | CDH, cervical myelopathy, cervical spondylotic radiculopathy, etc. |
*1 CDH : Cervical Disc Herniation
*2 CSCS : Cervical Spinal Canal Stenosis
*2 CSCS : Cervical Spinal Canal Stenosis
MECD/MECLMicroendoscopic Cervical Discectomy / Microendoscopic Cervical Laminectomy
Cervical spine surgery with endoscope according to MED/L
Both MECD and MECL are surgical procedures performed while viewing the surgical field with an endoscope. The patient is asked to lie face down on the operating table, and an incision is made in the back of the neck. The outer tube into which the endoscope is inserted is 16 mm in diameter, which results in a wound about 20 mm in size.| Indications | Cervical disc herniation, cervical spinal canal stenosis, cervical spondylosis, etc. |
|---|---|
| Method of anesthesia | General anesthesia |
| Length of hospital stay | 4-6 days |
| Wound size | Approx. 20 mm x one site |
FECFFull-endoscopic Cervical Foraminotomy
Cervical spine surgery with endoscope according to FED/L
FECF is a surgical procedure performed while viewing the surgical field with an endoscope. The patient is asked to lie face down on the operating table, and an incision is made in the back of the neck. The outer tube into which the endoscope is inserted is 7 mm in diameter, which results in a wound less than 10 mm in size. By removing the vertebral arch behind the nerve root, retraction of the nerve root can be avoided. If necessary, a herniated disc can also be removed from the back.
FECF is a type of surgical procedure called FESS (Full Endoscopic Spine Surgery). FESS uses a spinal endoscope, which is not easy for the surgeon to manipulate. Although there are only a limited number of doctors in Japan who can perform FESS, many of the doctors in our group are proficient in the procedure.
FECF is a type of surgical procedure called FESS (Full Endoscopic Spine Surgery). FESS uses a spinal endoscope, which is not easy for the surgeon to manipulate. Although there are only a limited number of doctors in Japan who can perform FESS, many of the doctors in our group are proficient in the procedure.
| Indications | Cervical disc herniation, cervical spondylotic radiculopathy, etc. |
|---|---|
| Method of anesthesia | General anesthesia |
| Length of hospital stay | 3-4 days |
| Wound size | 8-10 mm x one site |
Cervical laminoplasty
Surgical procedures indicated for many diseases of the cervical spine
Cervical laminoplasty is a procedure in which an incision is made in the vertebral arch and artificial bone is inserted to widen the narrowed spinal canal. This procedure does not use an endoscope. Endoscopic surgery is difficult when the narrowed area is extensive, in which case laminoplasty is indicated. The patient is asked to lie face down on the operating table, and a 50-80 mm incision is made in the back of the neck.| Indications | Cervical disc herniation, cervical myelopathy, cervical spondylotic radiculopathy, etc. |
|---|---|
| Method of anesthesia | General anesthesia |
| Length of hospital stay | 5-9 days |
| Wound size | 50-80 mm x one site |
Anterior cervical fusion
Surgical procedure performed from the front of the neck
Anterior cervical fusion surgery is a procedure in which a disc is removed from the side of the neck and the bone is shaved to relieve pressure on the nerves. A substitute materials is put in the space from where the disc was removed. The upper and lower bones fuse with each other over a period of six months to two years. The patient is asked to lie on his or her back on the operating table, and about a 30 mm incision is made on the lateral side of the neck. This method is suitable for conditions that are difficult to treat from behind, but must be performed with care to avoid touching vital organs such as the carotid artery, trachea, and esophagus.
| Indications | Cervical disc herniation, cervical spondylotic radiculopathy, cervical myelopathy, etc. |
|---|---|
| Method of anesthesia | General anesthesia |
| Length of hospital stay | 7-10 days |
| Wound size | 30 mm x one site |
Surgery of the Lower Extremities
Treatment types about our group's lower extremity surgeries
Treatment types about our group's lower extremity surgeries
For knee ligament and joint injuries resulting from sports or accidents, doctors at the Sports & Joint Center of Inanami Spine and Joint Hospital will perform surgeries.
| Operative procedure | Length of hospital stay | Indications |
|---|---|---|
| Anterior cruciate ligament reconstruction | 7-10 days | Anterior cruciate ligament tears and injuries. |
| Achilles tendon suture | 8-10 days | Achilles tendon ruptures and injuries. |
Anterior cruciate ligament reconstruction of the knee
Surgical procedures that have helped many athletes return to competition
Surgery is necessary for patients with an anterior cruciate ligament tear of the knee, especially if they play sports and want to maintain or improve their activity level in the future. Our group provides early rehabilitation after surgery in order to help patients return to their daily activities and sports as soon as possible. Patients can walk with two crutches the day after surgery, with one crutch on postoperative day 3, and with only a brace on postoperative day 5. Not only is it possible to get back to playing sports about 6 months after surgery, but there is little risk of re-tear or infection, and the overall postoperative outcome is excellent.
| Indications | Anterior cruciate ligament tears and injuries of the knee |
|---|---|
| Method of anesthesia | General anesthesia |
| Length of hospital stay | 7-10 days |
Achilles tendon suture
Developed a surgical method that is now used by many medical institutions
The “Uchiyama method of Achilles tendon suture” is a surgical procedure for Achilles tendon rupture developed by Dr. Eiji Uchiyama, a member of our group. This method, which was first presented by Dr. Uchiyama in 2004, is currently used for more than 600 cases a year at many health care facilities. Patients can get back to playing sports within 4 to 7 months after the surgery. Re-tears occurred in only 1 out of 137 patients between July 2015 and August 2021. Our group has had no cases of postoperative infection.
| Indications | Achilles tendon ruptures and injuries |
|---|---|
| Method of anesthesia | General anesthesia |
| Length of hospital stay | 8-10 day |